Rhino Husbandry Manual
Greater One Horned Rhinoceros
Health

This section provides a general overview of preventive medical and disease management, and chemical restraint of captive rhinoceroses. More detailed information for many of these topics is available in the references provided as well as through the Rhino Resource Center (www.rhinoresourcecenter.com).
Physiological Normals and Sample Collection
With the increased use of training for husbandry and medical procedures, resting values for heart rate, respiratory rate, temperature and other values have been obtained for non-restrained black rhinos. The various species appear to be similar with heart rates of 30 to 40 beats per minute and respiratory rates of six to 12 breaths per minute. Rectal temperatures are typically 34.5-37.5°C (94-99.5°F), although temperatures may be higher in anesthetized rhinos (37-39°C; 98.6-102°F) due to exertion or muscle tremors (Miller, 2003; Radcliffe and Morkel, 2007; Morkel et al., 2011). Values are comparable to domestic horse ranges. Limited information about electrocardiography (ECG) is available in rhinos (Jayasinge and Silva, 1972). Indirect blood pressure has been measured in unsedated black rhinoceros using a human blood pressure cuff around the base of the tail. Mean values reported for unanesthetized white rhino are 160 ± 2.9 mm Hg (systolic), 104 ± 2.3 mm Hg (diastolic), and 124 ± 2.2 mm Hg (mean blood pressure) (Citino and Bush, 2007). In anesthetized animals, etorphine can cause hypertension, although variable mean blood pressure measurements (107-280 mm Hg) have been observed, depending on drugs used and time values measured.
Hematologic, biochemical, mineral, protein electrophoresis, and blood gas values have been previously published (Tables 3.12-3.14; Flesness, 2002; Miller, 2003). Although most parameters can be generally interpreted similar to other perissodactyls, there are several differences that appear to be normal in rhinos. Total protein and globulins tend to be higher than in domestic horses. Other values that differ include lower sodium and chloride. Free-ranging rhinos tend to have higher creatine phosphokinase (CPK) than captive animals (this may be biased by immobilization technique)(Kock et al., 1990; Mathebula et al., 2012). Hypophosphatemia (low blood phosphorus) is a recognized problem in captive black rhinoceros, with levels dropping below 1 mg/dl. Low serum phosphorus (P) has been linked with hemolytic anemia and other blood disorder syndromes (Miller, 1993; Dennis et al., 2007). Oral and intravenous supplementation may be instituted in these cases. Anecdotal reports of doses used in black rhinos are 10 to 24 g elemental phosphorus (preferably chelated) orally once per day until normal serum levels are reestablished (E. Valdes, pers. comm.; Gillespie et al., 1990). In critical cases, intravenous sodium or potassium phosphate can be administered at 14.5 mmol P/hour but serum calcium should be carefully monitored.

Venipuncture can be routinely performed on awake captive rhinoceroses using training and/ or restraint devices (Fig. 3.8). The most commonly used sites for blood collection are the ear (auricular) vein, metacarpal vein (lower inside forelimb), and radial vein (inside of forelimb crossing the carpus)(Fig. 3.8-3.10). The tail (coccygeal) vein has also been used and is approached from the ventral aspect similar to the technique for blood collection in domestic cattle. plasma/serum banking, or for therapeutic phlebotomy (Mylniczenko et al., 2012). One to eight liters have been obtained from trained standing rhinoceros (Fig. 3.12; V. Clyde, pers. comm.). Rhinoceros blood cells resemble those of domestic horses. Nucleated red blood cells (NRBC) and reticulocytes may be observed in anemic animals. Elevated total white blood cell counts (wbc) and eosinophil numbers have been observed in wild rhinoceroses, presumably due to the response to capture and parasite loads, respectively.
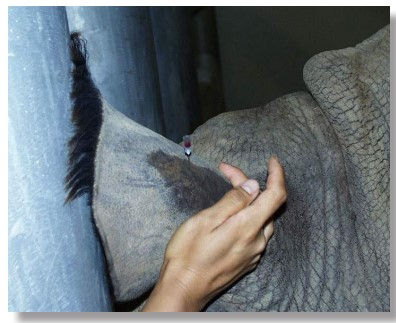



Fig. 4.7. Voluntary blood collection from auricular vein in awake rhinoceros
Fig. 4.8. Blood collection from the metacarpal vein in a standing rhinoceros.
Fig. 4.10. Arterial blood sample collection from medial auricular artery.
Fig. 4.9. Blood collection from radial vein in immobilized rhinoceros.
Urinalysis panels in captive rhinos are similar to horses with large numbers of calcium carbonate crystals, creating a normal milky yellow appearance to the urine. Calcium oxalate, phosphate, and ammonium crystals may also occur, depending on the diet. Occasionally dark discoloration of urine associated with pigmentation of certain browse species (e.g., ash, mulberry) can be mistaken for blood or myoglobin. However, analysis should be performed to rule-out any abnormalities. Normal values for the different rhino species have been published (Table 3.15; Haffey et al., 2008).
Due to size, cerebral spinal fluid collection has not been successful except in a few rhino calves (S. Citino, pers. comm.). Therefore, extrapolation of normal values from domestic horses and other perissodactyls should be used for interpretation.
Incorporation of scales into rhino facilities has permitted monitoring of body weights and physical condition. Regular weighing is recommended to observe trends associated with growth, diet changes, and disease. Average range for adult body weight is 800-1350 kg (1,764-2,976 lb; Miller, 2003).
Table 4.17. Reported range of mean urinalysis results from three captive rhinoceros species.
pH Specific Gravity
Greater Asian one-horned rhinoceros 8.08-8.70 1.019-1.031
Sumatran rhinoceros 8.16-8.32 1.010-1.021
Black rhinoceros 8.10-8.26 1.010-1.012
Preventive Medical Health Programs
Routine health monitoring should be performed on all rhinoceros on an ongoing basis. Animals should be trained to permit sampling and examination.
Additional tests are recommended to increase baseline information on other diseases to determine their significance to rhinoceros health. The final decision for specific procedures should be made by the animal care and veterinary staff based on individual circumstances.
-
Physical exam by a veterinarian familiar with rhinoceros health problems. This should include a review of all systems (if performed in a restraint device, exam may be limited by training and temperament of the individual and design of facility). Special attention for certain species include:
-
Greater Asian one-horned rhinos:
-
Foot exam due to prevalence of pododermatitis.
-
Ophthalmic exam for keratitis.
-
Nasal exam due to epistaxis.
-
-
-
Body weight—Actual weight should be recorded whenever possible; body scores and/or digital photos can be used when scales are not available.
-
Blood collection for complete blood count (CBC), serum chemistry panel, fibrinogen, serum protein electrophoresis and extra serum/plasma for banking (minimum of 10-20 ml). Blood smears should be carefully screened for the presence of hemoparasites, especially in recently captured or imported animals. The current Rhino SSP/TAG tissue/sample collection protocol should be consulted for additional samples that may be requested for research, disease screening, etc.
-
Fecal samples should be collected semiannually or at least annually (depending on management system) for direct, flotation, and sedimentation to detect internal parasites.
-
Annual enteric pathogen screening may be included, especially for animals in intensive management situations (e.g., breeding herd). Aerobic culture of feces for enteric pathogens should include special media for the detection of Salmonella spp. Because salmonella organisms may be shed intermittently, at least three to five fecal cultures should be performed (may be done on consecutive days).
-
Vaccinations—Annual vaccination for leptospirosis is recommended for greater one horned rhinoceroses. Vaccination for rabies, tetanus, and arboviruses (EEE/WEE/WNV) may be considered if the diseases are considered endemic in the area or increased risk factors are identified. There have been isolated cases of rabies and tetanus documented in rhinoceros (Jones, 1978; Mukherjee et al., 1984; Selvam et al., 2003). Check with the SSP veterinary advisor for the most current recommendations on species-specific vaccination protocols.
Additional preventive health recommendations have been included for consideration when performing examinations.
-
Serological screening for leptospirosis (multiple serovars) and West Nile Virus (WNV). Although these tests are not species-specific and have not been validated for rhinoceros, they may detect cross-reactive antibodies in exposed animals. The presence of antibodies does not necessarily denote current infection or disease. Antibodies to leptospirosis have been detected in vaccinated rhinoceros and may be used to monitor response and possibly determine frequency of vaccination, although data is insufficient to determine protective titers. Insufficient data is available at this time to determine the significance of WNV antibodies in rhinoceroses, although it is important to note that a greater one-horned rhinoceros with clinical signs developed a WNV titer during a period of known exposure (P. Calle, pers. comm.). One study in greater bone-horned rhinoceroses did not find seroconversion in response to vaccination with a commercial equine WNV vaccine (Wolf et al., 2008).
-
Serum/plasma vitamin E levels should be checked on a regular basis to assess adequacy of diet and supplementation protocols (see Nutrition chapter). Levels should be checked in any black rhinoceros with signs of illness. See the most current Rhino TAG/SSP preventive health protocol for recommended laboratories.
-
Reproductive tract examination—When feasible, a complete reproductive examination should be conducted to include transrectal ultrasound, semen collection and analysis, and serum or fecal collection for hormone analysis (Radcliffe et al., 1997). Uterine leiomyomas, cystic ovaries, and irregular cycling have been observed in captive animals (Hermes et al., 2004). Since these conditions can have potentially significant effects on reproduction, a careful evaluation is warranted if the animal is being considered for breeding. Standing laparoscopy enabled visual examination and uterine biopsy of a leiomyoma in a southern white rhinoceros (Radcliffe et al., 2000b). A number of publications describe the technique for ultrasonography in rhinoceroses and normal reproductive biology. The reader is referred to the Rhino Resource Center for further information (www.rhinoresourcecenter.com).
-
Urinalysis should include both fluid and sediment evaluation of a clean voided sample. Microbial culture should be considered if there is evidence of blood cells or bacteria.
-
Radiographs of feet are strongly recommended if any signs of pododermatitis or nail cracks are observed especially in greater one horned rhino (Atkinson et al., 2002). Regular foot trimming and care may require immobilization in certain individuals (i.e., those that have a history of chronic foot problems). See section on pododermatitis.
-
Diagnostic tests for tuberculosis—Periodic testing for tuberculosis in rhinoceroses should be considered, especially if there has been a history in the institution or herd. Intradermal testing can be performed using bovine PPD (0.1 ml ID) in the eyelid, behind the ear, caudal tailfold, or axillary region. Both false positive and false negative results have been found when performing intradermal tuberculin testing in rhinos (Godfrey et al., 1990). Ancillary tests such as nasal swabs, tracheal washes, and gastric lavages for mycobacterial culture have also been used. Serological tests [ElephantTB STAT-PAK®, MAPIA, DPP (dual pathway platform); Chembio Diagnostic Systems, Inc.] are being investigated for use in rhinos. See section on tuberculosis.
-
Other vaccination regimens will depend on regional requirements and exposure risks (consider multivalent vaccination for Clostridial diseases). Contact the SSP veterinary advisor for the most up-to-date information.
Animals being moved between institutions should receive a preshipment examination and testing. This is similar to the routine health procedures but should also include screening for tuberculosis and other requirements dictated by the receiving institution (see quarantine section below).
Neonatal Examinations
Ideally, neonates should be examined within 24 to 72 hours of birth to detect any congenital defects. Often the dam can be separated while the calf is manually restrained for a brief, but thorough exam, including body weight, and if feasible, blood collection. Complete blood count, biochemical panel, tests for passive transfer of immunoglobulins [e.g. glutaraldehyde coagulation, zinc sulfate turbidity, radial immunodiffusion plates (equine plates work well in rhinos and can be standardized by testing healthy rhinos), and serum protein electrophoresis], vitamin E level, and banking should be performed. A microchip may be placed behind the left ear for future identification. Particular attention during the exam should be paid to the umbilical stalk for signs of infection, urine leakage, or hernia; passage of meconium, normal rectal/anal anatomy and tone; suckling reflex and neurological status. Regular weights and developmental progress should be documented. Lack of weight gain may be due to inadequate maternal milk production and care, or an indication of health or developmental problems in the calf. GOH rhinoceros calves have been successfully hand-reared (covered under Nutrition chapter). In one case, a white rhinoceros calf was orphaned when its dam died, and the calf was taught to drink from a bucket at the age of six weeks. Weakness or other problems resulting in prolonged recumbency can cause decubital ulcers. Treatment of two neonatal white rhinos has been described using serial sedation with butorphanol alone or in combination with detomidine for restraint (Gandolf et al., 2006). Rectal prolapse has been reported in black rhinoceros calves, with surgical intervention required in at least two cases (Pearson et al., 1967; Abou-Madi et al., 1996). Leukoencephalomalacia has also been described in black rhinoceros calves (see disease section for more details)(Miller et al., 1987).
Parasites
Internal parasites are more commonly found in free-ranging rhinos than in captivity. Stomach botfly larvae (Gyrostigma pavesii) have been reported in black rhinoceroses (Velleyan et al., 1983). Other parasites reported include nematodes (Diceronema versterae, Parabronemia round— associated with stomach nodules), Draschia megastoma, multiple species of Kiluluma, Khalilia rhinocerotis and pinworms (Oxyuris karamoja). Tapeworms (Anoplocephala sp.) can cause asymptomatic infestation in both captive and wild rhinos (Miller, 2003). One case of neosporosis led to acute fatal myocarditis in a neonatal white rhino calf and abortion in another case (Williams et al., 2002; Sangster et al., 2010).
Ticks are regularly found on free-ranging rhinoceroses, and imported animals should be carefully examined and treated. Multiple species have been identified on African rhinos (Amblyomma hebraeum, Dermacentor rhinocerinus, Rhipicephalus maculates, R. muehlensi, R. simus, R. appendiculatus, R. zambeziensis, Haemaphysalis silacea, Hyalomma truncatum)(Penzhorn et al., 2008). Filarid (Stephanofilaria dinniki) and screwworms (Chrysomia bezziana) can lead to skin lesions in wild black rhinos, particularly prevalent in the axial region (Round, 1964; Penzhorn et al., 1994).
Vector-borne parasitic infections occur in endemic areas. Trypanosomiasis can infect black rhinoceros and lead to anemia in tsetse fly-endemic areas. Evidence of tick-borne disease has been documented in black rhinoceros due to Babesia bicornis sp. nov. and Theileria bicornis sp. nov. (Nijhof et al., 2003). In addition, antibodies to heartwater (Cowdria ruminantium) have been found in both African species where the Amblyomma ticks are present (Kock et al., 1992).
Capture and translocation or importation may exacerbate potential parasitic infestations and increase the risk of introduction of novel pathogens to a new environment. Therefore, careful screening for external and internal parasites, prophylactic treatment of wounds with fly repellant, pour-on tick treatments (coumaphos, flumethrin), and judicious use of antiparasitic medications (pyrantel pamoate, fenbendazole, ivermectin, praziquantel) should be considered. Check with the SSP veterinary advisor for current recommendations.
Quarantine
Due to the size, strength, and temperament of a rhinoceros, it may be logistically difficult to maintain isolation from other animals during arrival and quarantine. The Rhinoceros TAG/ SSP Recommended Preshipment Protocol for Rhinoceros lists a comprehensive battery of tests for health assessment prior to shipment. Since most zoological institutions will not have the facilities available to safely house and manage a newly arriving rhinoceros, it is important that the receiving institution work closely with the sending institution to ensure that all (or as many as possible) of the listed tests are conducted and results reviewed before shipment. Following the preshipment protocol may help compensate for some of the quarantine compromises that may be required. Regardless of preshipment test results, every attempt should be made to maintain some degree of physical separation of the incoming animal from the resident rhinos after arrival.
Current quarantine practices recommend a minimum 30 to 90 day quarantine period for most mammalian species in zoos and aquaria. Social concerns, physical facility design, and availability of trained rhino staff may dictate a modified quarantine protocol. Specific quarantine guidelines and protocols at each institution should be reviewed jointly and decisions made by the veterinary and animal management staff. Recommended procedures to consider as part of a comprehensive plan for rhinoceros quarantine include:
• Thorough physical examination including a review of all organ systems.
• Blood collection for CBC (including blood smear examination for hemic parasites), serum chemistry panel, fibrinogen, serum protein electrophoresis, and serum bank.
• Fecal collection for parasite screening (direct, flotation, sedimentation) conducted weekly for the first three weeks.
• Fecal cultures for Salmonella spp. conducted at least weekly for the first three weeks.
• Any procedures that were not completed prior to transport or that may be due, such as vaccination, serologic screening, or TB testing.
It should be emphasized that the quarantine test requirements should be strongly considered regardless of the results of preshipment testing. The stress of transport and quarantine may result in health changes (for example, Salmonella shedding) that were not detected during testing at the sending institution.
Hospitalization and Critical Care
In most cases, hospitalization is impractical with adult rhinoceroses. Most animals will be treated in their holding areas. Rhino calves may be hospitalized in adequate large animal holding facilities if the severity of their medical condition warrants. Barns or holding areas that incorporate species-appropriate restraint devices facilitate medical treatment. Some of the following medical problems require active intervention, including sedation, immobilization, injectable drug therapy, and/or fluid therapy. Although it has been achieved, fluid therapy in rhinoceros presents logistical challenges. In addition to the intravenous route, it is possible to improve hydration using rectal enemas with warm physiologic solutions or even tap water. Animal and staff safety should be a priority in any planned intervention.
Diseases
Tuberculosis
Mycobacterium bovis and M. tuberculosis have caused infections in captive rhinoceroses (Stetter et al., 1995; Miller, 2008). Although not currently reported in free-ranging rhinoceroses, there was a recent report of M. bovis infection in a black rhinoceros brought into captivity in South Africa (Espie et al., 2009). Initial infection may be asymptomatic or result in progressive weight loss and emaciation, with coughing and dyspnea occurring in the terminal stages. Nasal discharge may be present but is not a consistent sign. Most infections are pulmonary. Antemortem testing includes intradermal tuberculin test, tracheal and/or gastric lavage for mycobacterial culture, and serological tests (see preventive health section for details). Retrospective analyses of serum from M. tuberculosis-infected black rhinos showed positive results using the ElephantTB Stat-Pak® (Duncan et al., 2009). Treatment has been attempted using isoniazid, rifampin, ethambutol, and pyrazidamide (Barbiers, 1994; Duncan et al., 2009). However, assessment of successful response is limited. Concerns for other collection animals, staff and public health need to be considered prior to initiation of therapy. Since this is a reportable disease, notification of the appropriate state veterinary officials should occur promptly once a diagnosis is made. Consultation with the SSP veterinary advisor is also recommended.
Salmonellosis
Salmonella infection can cause enteritis and fatal septicemia in captive and newly captured wild rhinoceroses (Windsor and Ashford, 1972; Kenny et al., 1997). In a retrospective survey of captive black, white, and greater Asian one-horned rhinos in the U.S., 11% reported positive cultures, usually associated with clinical signs (Kenney, 1999). Research has shown that asymptomatic black rhinoceroses can carry and intermittently shed Salmonella in their feces (Miller et al., 2008). Clinical infection may result secondary to transport, changes in diet, immobilization, concurrent disease, or exposure to a large number of organisms. Lethargy, anorexia, signs of colic, diarrhea, and death may be observed. Successful treatment using trimethoprim-sulfamethaxozole and supportive care is possible if initiated early. However, treatment of asymptomatic animals is NOT recommended.
Leptospirosis
Leptospirosis usually presents with depression and anorexia. Other signs may include hemolytic anemia (not present in all cases), hemoglobinuria, signs of colic, and development of skin ulcers. Fatality rates are high in clinically affected black rhinos although successful treatment with trimethoprim-sulfamethaxozole and ceftiofur has been reported (Neiffer et al., 2001). Diagnosis is based on high antibody titers (microagglutination test – MAT) and confirmed by detection of leptospiral organisms in urine or tissues (fluorescent antibody test).Abortion has also been linked to infection with Leptospira in a greater one-horned rhinoceros (Miller, 2003) Preventive measures include annual vaccination of black rhinos with a multivalent large animal product, rodent and wildlife control programs, and good husbandry to minimize contamination of feed and water. Abscesses and systemic anaphylactic reactions, including hives and skin sloughing, have occurred following leptospirosis vaccination in the black rhinoceros. Those individuals with a history of systemic adverse reactions should forego regular vaccination.
Gastrointestinal Infections
See salmonellosis and GI torsion, impaction, and ulcers for other GI conditions.
Encephalomyocarditis Infection (EMC)
EMC viral infection usually results in acute death due to myocarditis (Gaskin et al., 1980). The southeastern/Gulf Coast states in the U.S. are considered an endemic area. Diagnosis is usually based on virus isolation at necropsy from heart, spleen, or other tissues (http://www.merckvetmanual. com/mvm/index.jsp?cfile=htm/bc/53600.htm). Prevention should target rodent control, although experimental vaccines have been proposed. A commercial vaccine is not currently available.
Fungal Pneumonia
Fungal pneumonia is usually due to Aspergillus spp. and primarily observed in black rhinoceroses secondary to immunocompromise from concurrent disease, broad spectrum antibiotic therapy, or corticosteroid use (Weber and Miller, 1996). Clinical signs may include weakness, weight loss, epistaxis, or other signs consistent with pneumonia. Diagnosis is challenging, although serology and bronchoscopy, with cytology and fungal culture, may be useful. Fungal pneumonia in the black rhinoceros is often associated with elevations in serum globulin, above levels generally observed in other chronic diseases (S. Citino, pers. comm.). Long-term treatment with antifungal drugs (e.g., itraconazole) is expensive and has unknown efficacy. Definitive diagnosis is often made at necropsy.
Anthrax
Death due to anthrax has been observed in wild rhinoceroses. Most cases result in sudden death. It has been implicated in a die-off of several Javan rhinos in Ujung Kulan National Park, though definitive diagnosis is often lacking in remote field regions (R. Radcliffe, pers. comm.) Foamy discharge from the mouth and nostrils can be seen and may appear similar to EMC infection. Diagnosis is based on identification of anthrax bacilli in blood or tissue smears. Vaccination of ranched rhinos has been used in some endemic areas of Africa. Sporadic outbreaks in domestic livestock occur in the U.S., although there have been no reports of rhino mortality in these areas (e.g., Texas).
Skin Conditions and Dermatopathy Syndrome
-
Neoplasia- A greater one-horned rhinoceros with SCC of the horn has also been successfully treated with surgery and radiation. (Greer et al., 2010). Cutaneous melanomas have been reported in both black and greater one-horned rhinoceroses (Wack et al., 2010)
-
Environmental—Dermatitis, especially in greater one-horned rhinos, may be due to inadequate access to wallows and pools. These cases illustrate the importance of biopsy and culture for identifying the etiology of and directing treatment in dermatologic cases in rhinos.
Pododermatitis and Chronic Foot Problems
Although all species of rhinoceros are susceptible to developing pododermatitis due to inappropriate substrate or other husbandry conditions in captivity, the greater one-horned rhino (GOHR) appears to be more susceptible to chronic foot problems. Studies comparing wild and European zoo GOHR revealed 41% had vertical and/or horizontal cracks, 16% had pad fistulas and ulcerations, 69% had abraded side horn walls associated with an inflammatory process, and all the captive breeding bulls and at least half of the females had cracks between the central sole and adjacent pad (von Houwald, 2005). In contrast, foot anatomy of the wild GOHR showed hard elongated and concave pads without lesions. The authors concluded that abrasive substrate, long-term indoor housing in northern climates, and limited access to a pool contributed to chronic foot trauma in captive rhinos. Over 28% of adult male captive R. unicornis are reported to have chronic pododermatitis (Atkinson et al., 2001). Management of the condition includes improvements in husbandry and medical/surgical interventions. Medical treatment may be in the form of oral antimicrobial medication and topical use of copper sulfate and oxytetracycline. Regular hoof trimming and surgical debridement of necrotic lesions, along with use of collagen products for granulation tissue stimulation, can lead to improvement in appearance and comfort of the animal. In addition to the factors mentioned above, nutritional imbalances (e.g., zinc) are also being investigated.
Corneal Ulcers and Keratitis
Corneal trauma and secondary infection can result in corneal ulceration and perforation. Surgical management of a melting corneal ulcer using a conjunctival graft has been described in a greater Asian one-horned rhino (Gandolf et al., 2000).
Horn Problems
Horn avulsion, cracks, or other trauma can occur as a result of acute or chronic rubbing, pressure, self-induced, or conspecific fighting. This may lead to myiasis, abscessation, osteomyelitis, or pain with behavioral changes. Radiographs, thermography, or fluoroscopy can be used to assess the extent of the damage. Treatment may involve debridement, antibiotics, wound treatment, and fly control (Suedmeyer, 2007). A squamous cell carcinoma of the horn in a greater Asian one-horned rhinoceros was diagnosed and managed with partial amputation and radiation therapy (Greer et al., 2010). The horn is attached to the basal dermal layer not unlike the laminae of the horse’s hoof wall and therefore perturbations in blood flow can presumably lead to laminitis. Please Sullivan paper on Vitamin A in appendix X.
Gastrointestinal Torsion, Impaction, and Ulcers and Other Conditions
Torsion may result from abdominal trauma or severe GI disease. Severe torsion may lead to acute death; other signs are related to abdominal pain. Dietary changes, dehydration, ingestion of foreign material (i.e., sand), and inadequate fiber content may result in GI impaction. Gastric ulcers have been observed on gastroscopy and at necropsy in rhinos that have received long-term non-steroidal therapy or have concurrent disease. A 32-year old black rhinoceros was euthanized due to rapid onset of wasting secondary to perforation of a pyloric ulcer and peritonitis. Treatment depends on identifying the cause and site of the gastrointestinal condition. Surgical correction of torsion is usually recommended, although most cases are not diagnosed prior to necropsy. Impaction can be treated using rectal enemas, oral administration of psyllium, mineral oil, or other products to increase GI water content. Equine anti-ulcer medications such as omeprazole, sucralfate, and H2-blockers have been used in rhinos by scaling the equine dose. Prevention includes adequate dietary fiber and fluid intake, and avoiding abdominal trauma and ingestion of foreign material. Esophageal dilation was observed in a black rhinoceros following ingestion of a foreign body; successful management involved diagnosis by endoscopy and a change in feeding practices to a low fiber diet (Radcliffe et al., 1998). Inflammatory bowel disease was confirmed at necropsy in a greater Asian one-horned rhinoceros that presented with weight loss and progressive diarrhea (Ferrell et al., 2010).
Gingivitis and Dental Tartar
All rhino species appear to accumulate dental tartar in captivity, especially if they are not given access to hard or course food items. However, black rhinoceros appear to develop severe proliferative gingivitis, not always directly associated with the degree of accumulation of calculus (Beagley et al., 2010). Lesions are vascular and periodically hemorrhage, causing blood-tinged saliva. The gross appearance is similar to raw ground meat. The cause of this condition is unknown but may be related to lack of browse in the diet. Similar to horses, rhinoceros also develop dental points that may eventually create clinical mastication problems with age and require periodic dental flotation.
Renal Disease
Since 2001, chronic glomerulonephritis and/or renal failure have been recognized as a contributing cause of death in at least seven black rhinos. Mineralization of other tissues has been associated with chronic renal changes as well as three cases of accidental vitamin D toxicosis (Murnane et al., 1994; Fleming and Citino, 2003). Weight loss, decreased appetite, dermatitis, and signs of gastroenteritis may be present, including gastric ulcers. Significant changes in blood urea nitrogen, creatinine or urinalysis were not always evident in these cases, making diagnosis difficult until necropsy. However, two white rhinos (aged >40 yr) both developed progressive chronic renal failure characterized by uremia, isosthenuria and hypercalcemia. Nutritional management using a high energy, low protein feed (Equine Senior, Purina Mills, St. Louis, MO, USA) was instituted in both cases and appeared to stabilize the renal disease (S. Ferrell and R. Radcliffe, pers. comm.). Further investigation into causes of renal disease (other than toxicosis-related) is needed.
Creosote Toxicosis
Seven fatalities occurred among a group of 20 black rhinoceroses captured and housed in bomas constructed with creosote-treated wood in Zimbabwe (Kock et al., 1994). Although five cases died after transport to the U.S. and Australia, they exhibited the same clinical signs and lesions as the initial cases. Animals were lethargic, partially anorectic, developed swollen limbs, and passed brown urine. Abnormal blood results included anemia, and elevated liver enzymes and bilirubin. Post-mortem findings included widespread hemorrhages; swollen, pigmented liver; and ulcers of the upper gastrointestinal tract. The presumptive cause of death was liver dysfunction due to creosote toxicosis. Exposure to creosote-treated housing materials should be avoided for all rhino species.
Common Injuries and Treatment: Skin Lacerations, Punctures, Wounds
Trauma due to conspecific fighting, mating injuries, collision with obstacles in enclosures or in crates, interspecific conflict or, in free-ranging situations, poaching is relatively common. Common sense application of wound treatment principles apply, although the thick skin does not lend itself to primary closure and has a tendency to undermine abscesses along the fascial planes. Therefore, wounds are usually treated by second intention using debridement, hydrotherapy, topical and/or systemic antibiotics, analgesics, and the array of wound healing products that accelerate granulation. A recent article describes the use of vacuum-assisted healing of a surgical wound in a black rhinoceros to improve healing time (Harrison et al., 2011).
Necropsy Protocol
Any rhinoceros that dies or is euthanized should have a complete necropsy performed and tissues submitted for histopathology. The Rhinoceros TAG/SSP Veterinary/Nutrition Blood and Tissue Collection Protocol for Rhinoceros should be consulted for current information on the species pathology advisors as well as specific sample requests for research and banking purposes. See Appendix for 2024 Rhinoceros Necropsy Protocol.
Capture, Restraint, and Immobilization Techniques
Management of captive rhinoceroses often requires procedures that involve handling of these large and powerful animals. Husbandry training techniques have advanced the application of preventive medical, diagnostic, and minor therapeutic procedures. However, intensive medical and surgical interventions may require physical and/or chemical restraint for safety and comfort of the patient and staff. Since new developments are continuously advanced in this field, the following recommendations should be used as guidelines, and the veterinary advisors and literature should be consulted for specific situations.
Physical Restraint
Advances have been made in facilities that include a variety of stall and chute designs for physical restraint of rhinoceros. These will be addressed in the Training and Enclosure Design chapters.
Chemical Restraint
Significant changes in options for chemical restraint of captive rhinoceroses have occurred during the last two decades. The degree of sedation, analgesia, or immobilization required will vary with the procedure to be performed. Health status and temperament of the individual animal, as well as facility design and staff experience may dictate preference for one technique over another.
Chemical Restraint and Anesthesia of Rhinoceros
Anesthesia of rhinoceroses requires adequate preparation, equipment, and experience. It is highly recommended that rhinoceros anesthesia should be attempted only with experienced personnel or after consulting knowledgeable practitioners. Contingency plans for emergencies are a key component of preparations. Clearly defined roles for all personnel should be outlined and reviewed. Adequate equipment for moving a large animal should also be available. The choice of chemical restraint techniques will be determined by a number of factors, including physical facilities where immobilization will be performed, health status of the individual, procedures to be achieved and level of analgesia required, length of intended immobilization, and experience of the veterinary and animal care staff. Only captive rhinoceros anesthesia techniques will be covered in this section. For more information on immobilization of free-ranging rhinoceros, the reader is referred to specific references on this subject (www.rhinoresourcecenter.com)(Miller, 2003; Bush et al., 2004; Portas, 2004; Kock et al., 2006; Radcliffe and Morkel, 2007; Wenger et al., 2007).
Equipment
With training and availability of physical restraint devices (“chutes”), drug delivery for chemical restraint can be more easily and accurately achieved, create less stress for the individual, and provide greater control of the induction. Standing restraint is also feasible in these situations. For rhinoceros in stalls, pens or exhibits, drug delivery often requires use of darting equipment. Depending on the situation, pole syringes with robust needles may be used on selected occasions. Hand-injection is also easily achieved in conditioned animals, although care must be taken when using potent opioids to ensure human safety. Most darting systems can be used in captive situations, as long as a robust needle (minimum 40-60 mm x 2 mm needle) is used to penetrate the thick skin and deliver the drug into the muscle. Nylon darts (Teleinject®, Telinject USA, Inc., Agua Dulce, CA, USA; Dan-Inject®, Danwild LLC, Austin, TX, USA) are preferred in these situations since they are less traumatic than metal darts. Ideal sites for drug injection are just caudal to the ear on the lateral cervical area, upper caudal hindlimb, or shoulder. However, any site can be used if the dart is placed perpendicular to the skin and is adequate to penetrate muscle. Additional equipment that should be available include a blindfold, ear plugs (cotton cast padding, stuffed socks), heavy ropes, and padding for recumbency. Inflated truck inner tubes can be used to reduce pressure points. Otherwise, heavy mats or padding should be used if the procedure will take place on a concrete floor. Immobilizations carried out in sandy or grassy areas may provide enough padding for shorter procedures. Contingency plans for moving a rhino that becomes recumbent in a difficult position should also be made. Lining stalls with plywood sheeting to prevent the head/horn from getting stuck should be considered in areas with open bollards or poles. Additional equipment should include the availability of oxygen and other emergency equipment. If a field procedure is being planned, an axe or chain saw and bolt cutter may be needed if there are trees/vegetation/other obstacles in the area where the rhino can get caught.
Preparations
Depending on the health status, environment, and procedure planned, removal of food and water prior to the procedure should be considered at least overnight. Consult the veterinarian for specific instructions.
Positioning
Rhinoceros are prone to developing myopathy and neuropathy after recumbency. The optimal position remains controversial and may be dictated by the planned procedure. Lateral positioning is often preferred since it provides the optimal circulation to the limbs, although sternal recumbency may provide better ventilation (Morkel et al., 2010). During the procedure, limbs should be “pumped” about every 20 minutes to encourage circulation (Radcliffe and Morkel, 2007). If the animal needs to be in sternal recumbency for the procedure, it is ideal to roll the animal into lateral recumbency whenever possible and pump the legs.
Anesthetic Monitoring
With the advent of new tools for monitoring physiological parameters in veterinary patients, it is imperative that monitoring be performed on immobilized rhinoceros to minimize complications. Ideally, an accurate weight or weight estimate will facilitate optimal drug calculation and prevent drug over- or under-dosing and associated complications (Adams et al., 2005). Thorough physical examination should be performed, along with regular recording of vital signs (respiratory rate and depth, heart rate, temperature, mucous membrane color and capillary refill time). Ideally, this should be assigned to dedicated personnel and measured at five-minute intervals throughout the procedure. Pulse oximetry is a useful tool for monitoring trends in hemoglobin oxygen saturation but can be prone to false readings due to placement and the thick skin of the patient. Therefore, it should not be a substitute for basic clinical assessment. Sites for placement of the sensor include the ear pinnae (scraping can sometimes improve readings) and mucosal folds of the penis, vulva, or rectum. Side-by-side placement of sensor pads has been used in the conjunctival sac, gingival and nasal mucosa, and inside the rectum, vagina, or prepuce. Ideally, readings should be greater than 90%, but interpretation should be made in conjunction with the color of the mucous membranes, blood, and other clinical signs. Capnography may also enhance patient monitoring by enabling early detection of adverse respiratory events, including hypoxia. While pulse oximetry gives trends in patient oxygenation, capnography provides information about CO2 production, pulmonary perfusion, alveolar ventilation, respiratory patterns, and elimination of CO2 from the anesthesia circuit and ventilator.
Standing Sedation
Standing sedation should only be attempted under conditions that take into consideration animal and staff safety. The type of procedure, as well as the temperament of the animal, restraint device, and husbandry training of the individual, will determine the level of sedation and analgesia required. Excitement and environmental or painful stimuli can override drug effects. As a general rule, individuals that are acclimated to people and husbandry training and restraint practices tend to require lower doses of immobilizing agent. Opioids tend to have more potent effects than the tranquilizer/sedative classes of drugs. A combination of butorphanol and azaperone has proven effective for repeat procedures, inducing standing sedation and recumbency in the white rhinoceros (Radcliffe et al., 2000a). See Table 3.16 for suggested doses for standing sedation of captive rhinoceros.
Table 3.16 Standing chemical restraint doses for captive GOH rhinos
Chemical Restraint Drug(s) Reversal Agent(s)
100 mg butorphanol + 100 mg azaperone IM naltrexone at 2.5 mg/mg butorphanol
0.5-1.5 mg etorphine IM naltrexone at 40 mg/mg etorphine
Immobilization/General Anesthesia
The primary class of drugs for general anesthesia in rhinoceros is the opioids. Etorphine is most commonly used, although carfentanil and more recently, combinations of etorphine and thiafentanil have also been administered to rhinos. Opioids are typically combined with azaperone, an alpha-2 agonist (e.g., xylazine, detomidine), or acepromazine to provide muscle relaxation and to counteract the hypertensive effect of the opioids (LeBlanc et al., 1987). Midazolam, diazepam, or guiafenisen infusion can also provide additional muscle relaxation. Greater one-horned rhinos appear to be more sensitive to the effects of opioids than black rhinos and exhibit muscle tremors, limb paddling, hypoxia, hypercapnia, and hypertension (Atkinson, 2001; Portas, 2004). Butorphanol has been administered to antagonize respiratory depressive effects in white rhino (10-20:1 butorphanol:etorphine in mgs); however, it may also lighten the plane of anesthesia (Miller et al., 2013). Other partial opioid agonist-antagonists are routinely used in the field and can be adapted for captive rhinos when available (e.g., nalbuphine). Butorphanol-azaperone and butorphanol-medetomidine/detomidine combinations have successfully induced recumbency in captive greater one-horned rhinos (Portas, 2004; Radcliffe et al., 2007; Waltzer et al., 2010).
Supplemental ketamine, opioids, guifanesin, propofol, or isoflurane can be used to deepen the level of anesthesia and lengthen immobilization as required (Ball et al., 2001). See Table 4.19 for recommended doses used for recumbent immobilization of rhinoceros. Oxygen supplementation by intratracheal intubation or nasal insufflation (flow rates of 15-30 liters/minute) can increase oxygen saturation values (Morkel et al., 2010). Doxapram administration for apnea has also been used in rhinos but may only provide short-term relief. Partial or complete reversal should be considered in severe cases of hypoxia.
Use of Tranquilizers/Sedatives for Transport and Other Uses
There may be occasions other than medical procedures when rhinoceros need to be sedated for short or more extended periods of time, such as during crating and transport, or confinement for other reasons. With the advent of husbandry training, the need for drugs in captive rhinos has become more limited but should always be available as an option. Tranquilizer/sedative drugs may be used in rhinoceroses to relieve anxiety, reduce hostility, decrease motor activity, alleviate excitement, and to facilitate animal introductions. Drug choice is based on the desired duration of action and expected outcome. For short duration tranquilization/sedation, benzodiazepines (2-6 hr; adult doses: midazolam 25-50 mg IM; diazepam 20-30 mg IM) and azaperone (2-4 hr; 80-200 mg IM) are useful choices in black rhinoceros. Long-acting neuroleptics (LANs) are typically administered in free-ranging rhino after capture for transport and boma acclimation, although they have also been used in captive rhino for longer duration tranquilization.
Table 4.19. Recumbent immobilizing doses for adult captive greater one-horned rhinoceros.
Drug(s) Reversal Agent(s)
3.5-3.8 mg etorphine + 14 mg detomidine + 400 mg ketamine IM naltrexone 50 mg/mg etorphine atipamezole 5 mg/mg detomidine
2.5 mg etorphine + 10 mg acepromazine IM naltrexone 50 mg/mg etorphine ½ IV, ½ IM
0.7-1 mg carfentanil IM naltrexone 100 mg/mg carfentanil
120 mg butorphanol + 80 mg detomidine naltrexone 2.5 mg/mg butorphanol
atipamezole 5 mg/mg detomidine
Fig. 4.1 A black rhino foot crack with bruising on sole.
